
Fitness
Where and why is mpox disease spreading in the DRC?

The Democratic Republic of Congo (DRC) is experiencing the biggest outbreak of the viral mpox disease ever recorded, with tens of thousands of people infected as of June. In December 2022, the government declared it an epidemic.
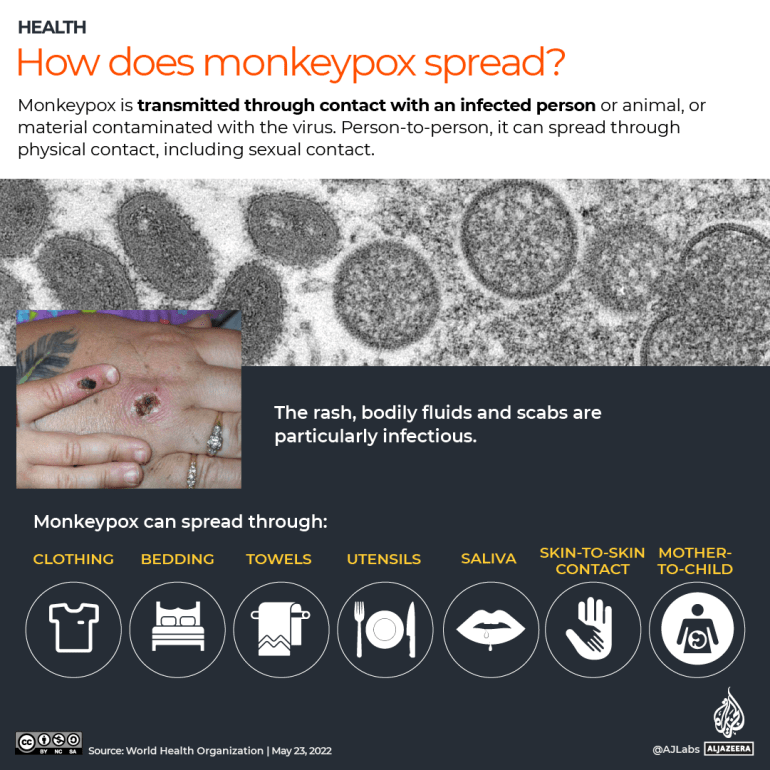
Formerly called monkeypox, the mpox disease is caused by the monkeypox virus, and is typically zoonotic – that is, it can be transmitted from animals to humans.
The virus is endemic to the densely forested regions of Central and West Africa and is related to the virus that caused the now-eradicated smallpox. Mpox can prove fatal in severe cases, with the primary symptoms being an itchy rash all over the body and a fever. Vaccines can limit infection.
Although outbreaks are common in the DRC, health experts said a new strain has been discovered this time in one part of the country.
Here’s what we know about the outbreak:
When did the mpox outbreak start?
The epidemic began in May 2022 in the country’s eastern Kwango province. However, it has since spread to 22 of DRC’s 26 provinces, including the capital, Kinshasa.
Transmission is still concentrated in the east, however, with a high spread recorded in Kamituga, a mining town in the eastern South Kivu province. Doctors have found a new strain of the virus in the town.
Since 2022, more than 21,000 cases have been reported with more than 1,000 deaths, according to the World Health Organisation (WHO). In 2023, a total of 14,626 cases and 654 deaths were recorded.
This year alone, 7,851 cases had been reported by the end of May, with 384 deaths. Many of those infected are children under five (39 percent). Close to two-thirds (62 percent) of those dying from the disease are also children.
The country’s Equateur, Sud Ubangi, Sankuru and South Kivu provinces are among those which have been hit the worst.
How many variants of mpox are there and how deadly are they?
There have always been two mpox types, also known as clades.
Clade 2 is less deadly. It is the type that was spread in a 2022 outbreak first recorded in London and that reached 111 countries in Europe, South and North America, Africa, the Middle East, Asia and Oceania. More than 99 percent of people infected in that epidemic survived because that clade of the virus is less deadly. Rich countries affected by the outbreak were also able to stockpile vaccines and anti-virals for treatment.

The clade 1 classification, however, is much more severe, and could kill up to one-tenth of people infected. It is clade 1 that has usually cropped up in the DRC, and is causing the current outbreak.
This clade of the virus has typically spread through normal physical contact. However, infections are being spread mostly through sexual contact in this outbreak, experts have said.
That is particularly true in the hotspot town of Kamituga, which has a large population of sex workers, said Dr Jean Bisimwa Nachega, a professor of medicine at Pittsburgh University.
Kamituga is the same location where the new strain of the Clade 1 classification was discovered in September 2023.
It is a “significant development”, Dr Nachega said, referring to the vulnerabilities of sex workers, who, in addition to being economically disadvantaged and lacking access to healthcare, are also more likely than the rest of the population to have compromised immunity from diseases like HIV.
“Unlike historical animal-to-human transmission, human-to-human sexual transmission, especially among high-risk groups like sex workers, adds a new challenge to controlling the virus,” he said.
The WHO says it’s unclear if this variant is more transmissible or if it leads to more severe sickness.
Doctors speaking to The Associated Press said the new variant is presenting differently. Usually, mpox lesions appear on the face, arms, chest and legs, and are clearly visible on an infected person. In this case, however, the lesions being reported are largely on the genitals, experts said, making it much harder to track and diagnose cases.
There were no documented cases of sexual transmission of the clade I virus in past DRC outbreaks, according to WHO. Cases in the country reported since the 1970s, have been understood to be primarily due to ordinary direct contact with infected persons or animals.
What are the main obstacles the authorities are facing?
The eastern region of the DRC is also badly affected by continuing conflict and is limited in resources, making it harder for authorities to adequately track, treat and monitor infected people, experts said. There are only two testing laboratories in Kinshasa and Goma, and only 18 percent of reported cases have been tested in labs.
The WHO has said there are also insufficient treatment kits in the country, and virtually no vaccines. Tecovirimat, an antiviral that was authorised for smallpox is being tested on more vulnerable patients in the DRC, according to WHO.
Vaccines can help with minimising the spread and were crucial in containing the outbreak in 2022 that affected wealthier countries, such as the United Kingdom and United States. But there are not enough vaccines to cover DRC’s 100 million population. The country’s minister of health has authorised doctors to administer the vaccines that are available in the highest-risk areas. Officials said the DRC is in talks with countries, including Japan, in a bid to procure more vaccines.
Public awareness about mpox is also limited, making self-reporting and containment difficult. Some patients have left isolation to buy food or continue their professional activity, experts said.
The fact that the disease can now be sexually transmitted brings an added layer of stigma, a problem which dogged healthcare staff during the initial spread of HIV/AIDS, experts pointed out. Experts said there is a risk of “silent transmission” if people don’t come forward themselves.

What are the risks for other African countries?
The eastern region of DRC which shares borders with Rwanda, Burundi, Uganda and Tanzania, is also a highly transient place, with people moving in and out regularly, increasing the risk of transmission to other countries. To the south, DRC borders Zambia and Angola, while its western and northern regions share borders with the Republic of Congo, the Central African Republic and South Sudan.
Like the DRC, many other African countries also have limited testing capacity, treatment and surveillance capabilities, making this an issue of regional and global concern, Dr Nachega said.
“Infectious diseases do not respect borders. Outbreaks in one region can quickly spread to other parts of the world, as seen with COVID-19. Even though the current mpox outbreak appears to be contained in one part of the DRC, people across the continent should remain vigilant,” he added.
So far, 19 cases have been detected in the neighbouring Republic of Congo, believed to have been spread from the DRC – although this has not been confirmed. In April, authorities there declared a public emergency.
Further afield, in Cameroon, 23 cases of the clade 2 virus were reported between January and April this year. South Africa has also recorded five clade 2 cases in an outbreak between January and May, although WHO says there may be more non-documented cases.
These cases are likely not directly related to the DRC outbreak. There’s frequent travel between South Africa and the DRC for trade but the cases are believed by some experts to be linked to the global clade 2 outbreak from 2022.

20/7/2024 Horse Racing Tips and Best Bets – Rosehill, Winter Challenge day
 "BCCI want Test specialists to play domestic cricket; Rohit, Virat, Bumrah to be exceptions")
BCCI want Test specialists to play domestic cricket; Rohit, Virat, Bumrah to be exceptions

HORSE RACING DAY 5: Andrew Champagne’s picks, analysis, bankroll
HORSE RACING DAY 5: Andrew Champagne’s picks, analysis, bankroll

600 Jobs, 25,000 Seekers: Air India Drive Sets Off Stampede Fear In Mumbai

More Trips, Higher Prices: Business Travel Spending May Finally Top 2019 Levels

Let’s take this offline: why indie fashion boutiques are back in fashion

Blue Jays balance college-heavy Draft with a few high-upside picks

Get to Know Gopher Men’s Basketball’s Frank Mitchell – University of Minnesota Athletics
