
Fitness
Landmark Analysis of ENZAMET (ANZUP 1304)
")
(UroToday.com) The 2024 American Society of Clinical Oncology (ASCO) annual meeting held in Chicago, IL was host to the Poster Session: Genitourinary Cancer: Prostate, Testicular, and Penile. Dr. Ronan McLaughlin discussed the prognostic implications of PSA levels at 7 months in metastatic hormone-sensitive prostate cancer treated with enzalutamide, presenting a landmark analysis of ENZAMET (ANZUP 1304).
ENZAMET (NCT02446405) is an international, open label, randomized, phase 3 trial conducted at 83 sites across Australia, Canada, Ireland, New Zealand, the UK, and the USA. Participants were males aged 18 years or older diagnosed with metastatic, hormone-sensitive prostate cancer with an Eastern Cooperative Oncology Group performance status score of 0-2. Participants were randomly assigned in a 1:1 ratio to androgen deprivation therapy (ADT) combined with oral enzalutamide (160 mg once daily) or a standard oral non-steroidal antiandrogen (bicalutamide, nilutamide, or flutamide) until clinical disease progression or prohibitive toxicity. ENZAMET showed that enzalutamide added to ADT with or without docetaxel improves overall survival (OS) compared with ADT plus standard non-steroidal anti-androgen (NSAA).1
Additionally, in an exploratory analysis of CHAARTED, a PSA level of ≤ 0.2 ng/mL at 7 months served as a prognostic indicator for extended OS in metastatic hormone-sensitive prostate cancer (mHSPC), regardless of docetaxel administration.2 Similarly, the SWOG 9346 study, compared continuous versus intermittent ADT in patients with mHSPC.This trial showed that patients achieving a 7-month PSA ≤ 0.2 ng/mL experienced significantly longer survival compared to those who did not reach this PSA level.3
Dr McLaughlin noted that for this study they assessed PSA levels in ENZAMET participants at 7 months after randomization, regardless of the prognostic subgroup or treatment arm. Bottom of FormParticipants were included if they were followed for at least 7 months after randomization and had availability of PSA and OS outcome data. This landmark analysis at 7 months used the prognostic classifiers previously identified in SWOG 9346 and CHAARTED (2,3) of PSA ≤ 0.2 and > 0.2 at 7 months after initiation of therapy. The investigators used LASSO penalization to construct a multivariable model for PSA ≤ 0.2 ng/mL at 7 months.
Of the 1,125 patients in the ENZAMET study, 57% had a PSA ≤0.2 ng/mL at 7 months. Among them, 271 out of 562 (48%) were in the NSAA arm, compared to 375 out of 563 (67%) in the Enzalutamide arm. A total of 1,104 participants were included in the landmark analysis at 7 months. Among these patients, baseline characteristics, including age, volume of disease, and planned docetaxel, were similar between both groups.
In the ADT + NSAA (+/- Docetaxel) group 49% achieve a PSA ≤0.2ng/mL, compared to 68% in the ADT + Enzalutamide (+/- Docetaxel) group. The five-year OS for ADT + NSAA (±Docetaxel) arm was 71% for patients who at 7 months had a PSA ≤ 0.2 versus 36% for those whose PSA was > 0.2. For the ADT + Enzalutamide (±Docetaxel) arm the OS was 74% if the PSA ≤ 0.2 vs. 43% if the PSA was > 0.2.
The landmark analysis of OS in high-volume patients was consistent with the primary results. Regardless of the treatment arm, patients who achieved a PSA ≤ 0.2 at 7 months had significantly improved overall survival. Additionally, regardless of whether Docetaxel was used, PSA ≤ 0.2 at 7 months remained significantly associated with survival in both treatment groups.
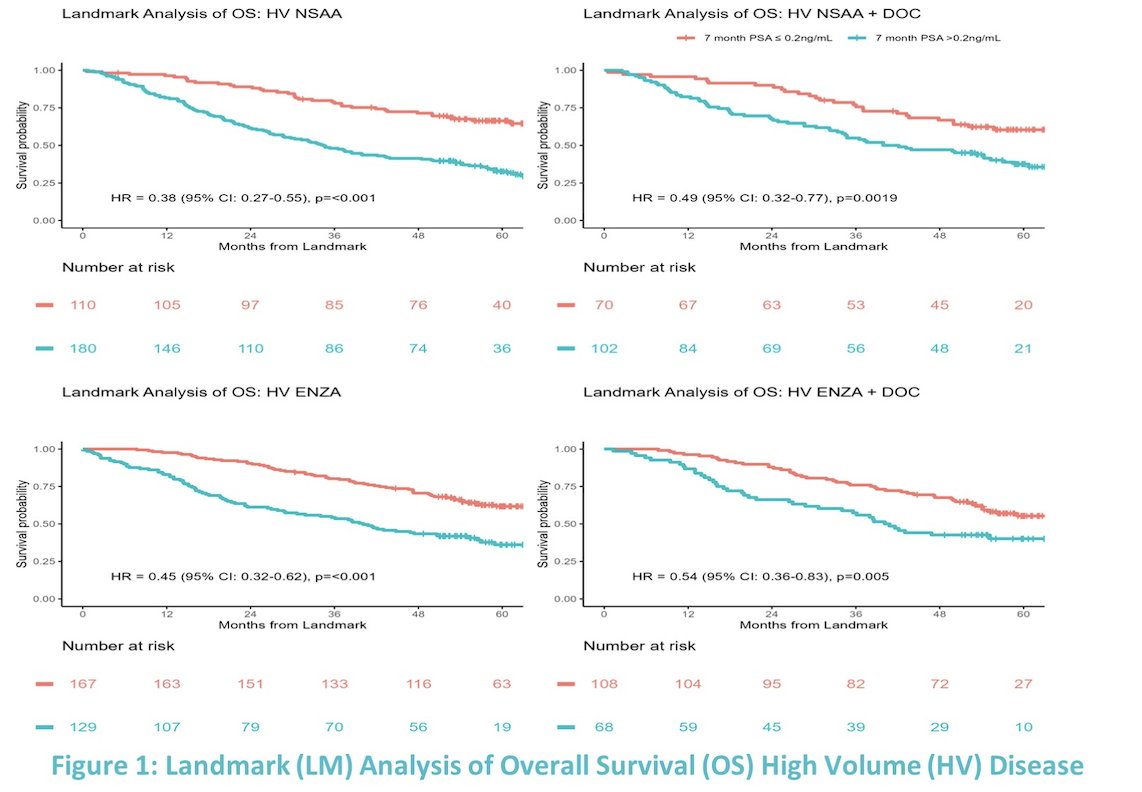
Similarly, PSA ≤ 0.2 at 7 months was associated with significantly improved overall survival in patients with low volume mHSPC who were treated with ADT + NSAA or ADT + Enzalutamide. However, this landmark analysis showed that in patients with low-volume disease who were also treated with docetaxel, PSA ≤ 0.2 at 7 months was no longer significantly associated with OS.

The percentage of pts with PSA levels at 7 months ≤0.2ng/mL and corresponding 5-year OS outcomes by metastatic burden, outlining treatment arm ± docetaxel is outlined in the table below. Of note, the 5-year OS was almost doubled regardless of the treatment arm, in the patients who achieved a PSA of ≤0.2ng/mL at 7 months.

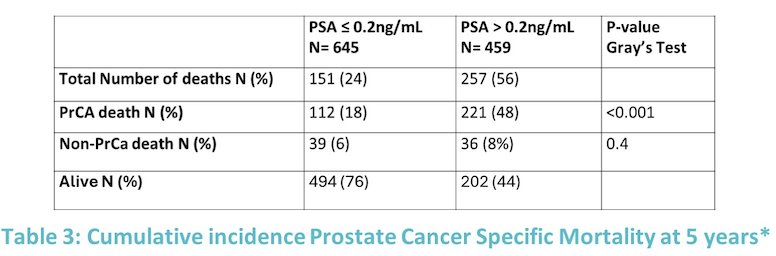
Prostate cancer-specific mortality using competing risk analysis was assessed for PSA ≤ 0.2 ng/mL vs. PSA > 0.2 ng/mL at 7 months. Overall, among patients who achieved a PSA ≤ 0.2 ng/mL at 5 years, 18% experienced prostate cancer-related deaths, compared to 48% in those whose PSA was > 0.2 ng/mL.

Concluding his presentation, Dr. McLaughlin conveyed the following key takeaways:
- This post-hoc analysis of ENZAMET demonstrated that a PSA nadir of ≤0.2 at 7 months is associated with a longer 5-year OS regardless of treatment arm and metastatic burden in ENZAMET.
- Enzalutamide increased the rate of achievement of PSA ≤0.2 for all groups of participants.
- Participants who achieve a PSA of ≤0.2 at 7 months are less likely to die from prostate cancer (p
Presented by: Ronan Andrew McLaughlin, MD, MRCPATH, MBBCh, Clinical Fellow at the Princess Margaret Cancer Centre, University Health Network, University of Toronto, Canada.
Written by: Julian Chavarriaga, MD – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @chavarriagaj on Twitter during the 2024 American Society of Clinical Oncology (ASCO) annual meeting held in Chicago, IL between May 31st and June 4th.
References:
- Sweeney CJ, Martin AJ, Stockler MR, Begbie S, Cheung L, Chi KN, Chowdhury S, Frydenberg M, Horvath LG, Joshua AM, Lawrence NJ, Marx G, McCaffrey J, McDermott R, McJannett M, North SA, Parnis F, Parulekar W, Pook DW, Reaume MN, Sandhu SK, Tan A, Tan TH, Thomson A, Vera-Badillo F, Williams SG, Winter D, Yip S, Zhang AY, Zielinski RR, Davis ID; ENZAMET trial investigators and Australian and New Zealand Urogenital and Prostate Cancer Trials Group. Testosterone suppression plus enzalutamide versus testosterone suppression plus standard antiandrogen therapy for metastatic hormone-sensitive prostate cancer (ENZAMET): an international, open-label, randomised, phase 3 trial. Lancet Oncol. 2023 Apr;24(4):323-334. doi: 10.1016/S1470-2045(23)00063-3. PMID: 36990608.
- Harshman LC, Chen YH, Liu G, Carducci MA, Jarrard D, Dreicer R, Hahn N, Garcia JA, Hussain M, Shevrin D, Eisenberger M, Kohli M, Plimack ER, Cooney M, Vogelzang NJ, Picus J, Dipaola R, Sweeney CJ; ECOG-ACRIN 3805 Investigators. Seven-Month Prostate-Specific Antigen Is Prognostic in Metastatic Hormone-Sensitive Prostate Cancer Treated With Androgen Deprivation With or Without Docetaxel. J Clin Oncol. 2018 Feb 1;36(4):376-382. doi: 10.1200/JCO.2017.75.3921. Epub 2017 Dec 20. PMID: 29261442; PMCID: PMC5805480.
- Hussain M, Tangen CM, Berry DL, Higano CS, Crawford ED, Liu G, Wilding G, Prescott S, Kanaga Sundaram S, Small EJ, Dawson NA, Donnelly BJ, Venner PM, Vaishampayan UN, Schellhammer PF, Quinn DI, Raghavan D, Ely B, Moinpour CM, Vogelzang NJ, Thompson IM Jr. Intermittent versus continuous androgen deprivation in prostate cancer. N Engl J Med. 2013 Apr 4;368(14):1314-25. doi: 10.1056/NEJMoa1212299. PMID: 23550669; PMCID: PMC3682658.

20/7/2024 Horse Racing Tips and Best Bets – Rosehill, Winter Challenge day
 "BCCI want Test specialists to play domestic cricket; Rohit, Virat, Bumrah to be exceptions")
BCCI want Test specialists to play domestic cricket; Rohit, Virat, Bumrah to be exceptions

HORSE RACING DAY 5: Andrew Champagne’s picks, analysis, bankroll
HORSE RACING DAY 5: Andrew Champagne’s picks, analysis, bankroll

600 Jobs, 25,000 Seekers: Air India Drive Sets Off Stampede Fear In Mumbai

More Trips, Higher Prices: Business Travel Spending May Finally Top 2019 Levels

Let’s take this offline: why indie fashion boutiques are back in fashion

Blue Jays balance college-heavy Draft with a few high-upside picks

Get to Know Gopher Men’s Basketball’s Frank Mitchell – University of Minnesota Athletics
